Adenomyosis Treatment in Dubai
Adenomyosis Treatment
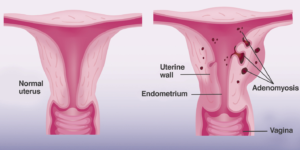
Adenomyosis is a condition in which the cells that line the inside of the uterus (endometrium) are abnormally located in the uterine wall (myometrium). This condition can result in enlarged uterus. This tissue thickens, breaks down, and bleeds during every menstrual cycle and can cause very painful periods and heavy bleeding. Adenomyosis can be difficult to diagnose and, without seeing a specialist, symptoms like heavy bleeding and pelvic pain are often dismissed.
Adenomyosis Symptoms
Adenomyosis can vary greatly from woman to woman. It can be localized (to one area of the uterus), diffuse (involving large areas of the uterine muscle), scattered, or clustered. Adenomyosis can cause debilitating pain and severe menstrual bleeding for some women; however, up to 30 percent of women with adenomyosis have no symptoms at all.
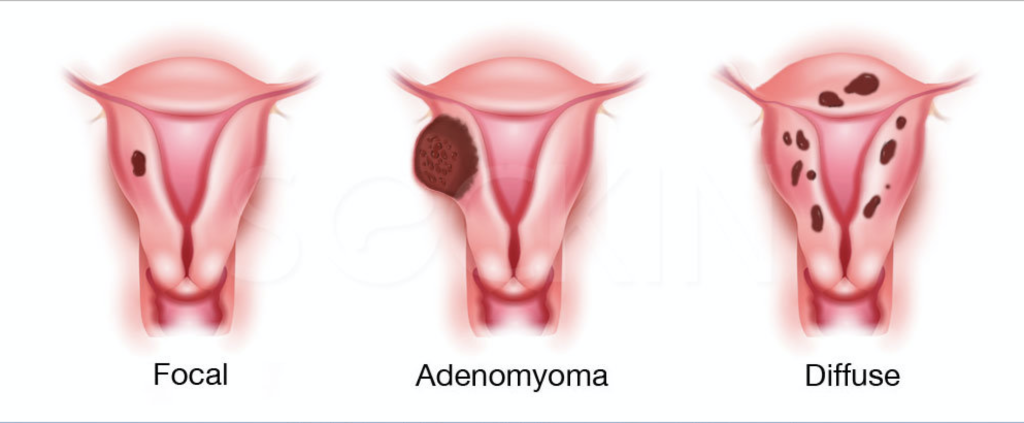
Types of Adenomyosis
Adenomyosis Risk Factors
It seems that childbearing, previous uterine surgery, short menstrual cycles, and an early age of first period may be risk factors for adenomyosis.
Coexistence with other Gynecological conditions
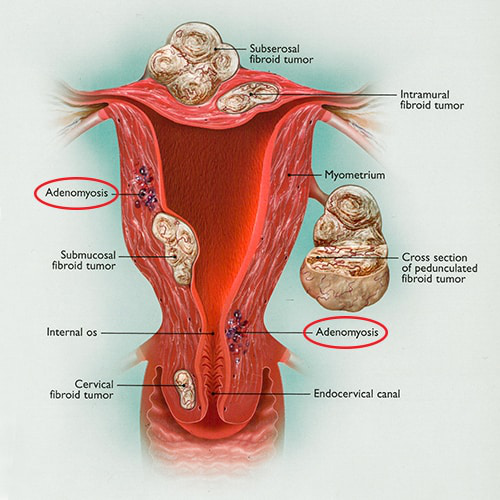
Adenomyosis frequently coexists with other gynecological diseases, such as endometriosis and uterine fibroids. In 15% to 57% of cases, uterine leiomyomas and adenomyosis coexist in the same uterus and women with both conditions are more likely to experience pelvic pain
Adenomyosis and endometriosis share a number of features, so that for many years adenomyosis has been called endometriosis interna. Nevertheless, they are considered two different entities because of specific pathogenic pathways and clinical presentation, although they often coexist in the same patients. Adenomyosis prevalence in women with endometriosis ranges from 20% to 80%.
Impact on Fertility
Adenomyosis has been considered the typical uterine condition of multiparous women, although an increasing amount of evidence suggests an association with infertility and reproductive failure. In a recent study on infertile women, adenomyosis prevalence were 24.4% in women at least 40 years old and 22% in women less than 40 years old. This percentage increased to 38.2% in cases of recurrent pregnancy loss and to 34.7% in previous ART failure.
Currently, infertility is considered one of the possible clinical presentations of adenomyosis and several theories have been proposed to explain the underlying mechanisms. Abnormal utero-tubal transport seems to be an important mechanism leading to infertility and is due to anatomical distortion of the uterine cavity but also to disturbed uterine peristalsis and sperm transport. The inner myometrium present with dysfunctional hyperperistalsis and increased intrauterine pressure. In addition, in the presence of adenomyosis, ultrastructural myometrial abnormalities cause a disturbance in normal myocyte contractility with subsequent loss of normal rhythmic contraction
HOW DO WE DIAGNOSE?
Clinical suspicion is the key to diagnosis. Women with adenomyosis typically complain of heavy menstrual bleeding and severe period pain. The uterus can be enlarged and tender.
Transvaginal ultrasound sonography represents the first-line imaging technique to diagnose adenomyosis as it is widely available, relatively inexpensive, and very accurate if performed by expert sonographers.
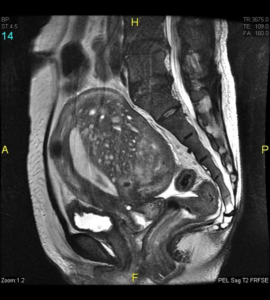
MRI is more accurate than transvaginal ultrasound, especially when the adenomyosis is superficial or diffuse, and when coexisting fibroids maybe confused with focal adenomyosis

Adenomyosis Treatment
Adenomyosis has a negative impact on women’s quality of life in a high percentage of cases because of abnormal uterine bleeding and pain requiring a lifelong management plan through medical or surgical treatment. The choice depends on the woman’s age, reproductive status, and clinical symptoms. However, so far, few clinical studies focusing on medical or surgical treatment for adenomyosis have been performed, and no drugs labelled for adenomyosis are currently available. Nonetheless, the disease is increasingly diagnosed in young women with reproductive desire, and conservative treatments should be preferred.
The only cure for adenomyosis is a hysterectomy but minimally invasive surgical treatments should be performed in specific cases especially in symptomatic women who is young and wishing to conserve fertility. Conservative surgical options include hysteroscopic endometrial and adenomyoma resection, laparoscopic resection of adenomyosis, high-intensity focused ultrasonography, and uterine artery embolization. Unlike fibroids, which are often surrounded by a capsule, there is no clear border between adenomyotic tissue and normal uterine tissue. Because of this, adenomyosis cannot be effectively removed the way fibroids can, and, when removed, portions of the uterine muscle are removed as well.
Choosing a GYN Specialist for surgical adenomyosis treatment
When it comes to lesser known GYN conditions like adenomyosis, women should seek a specialist for optimal care. Adenomyosis surgery should be performed by a skilled laparoscopic surgeon with immense experience in this field.